Alzheimer's disease, AD, is defined in part by the buildup of amyloid plaques made from the 42-residue amyloid-β peptide, Aβ42. The aggregation cascade behind those plaques begins long before symptoms appear, opening a window for early intervention. Glucagon-like peptide-1 receptor agonists, GLP-1RAs, are widely prescribed for type 2 diabetes and weight management, and observational data link their use to lower rates of all-cause dementia. A phase 2b trial further found that liraglutide slowed brain volume loss and cognitive decline in mild-to-moderate AD patients relative to placebo. Molecular evidence that GLP-1RAs act directly on Aβ42 aggregation, though, has been sparse.
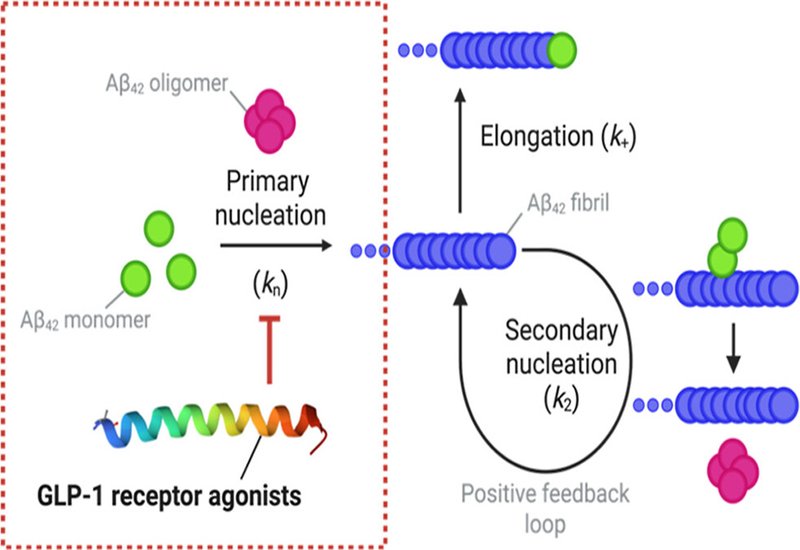
Researchers in the Limbocker Lab at the United States Military Academy, West Point, published in J. Am. Chem. Soc., combined thioflavin-T kinetics, Congo red fluorescence, atomic force microscopy, AFM, dynamic light scattering, and FTIR to dissect how five FDA-approved GLP-1RAs, semaglutide, tirzepatide, liraglutide, exenatide, and dulaglutide, affect distinct microscopic steps of Aβ42 fibril formation. Global fitting with the AmyloFit platform, across unseeded, 5%-seeded, and 25%-seeded reactions, let the team assign separate potencies for primary nucleation, secondary nucleation, and elongation.
Semaglutide and tirzepatide each lengthened the aggregation lag phase without changing the growth-phase slope, the kinetic signature of selective primary nucleation inhibition. Fits perturbing only primary nucleation reproduced the data, giving IC50 values for primary nucleation, KIP, of 0.422 μM and 0.325 μM. Seeded assays showed neither compound meaningfully touched secondary nucleation or elongation, and the resulting fibrils matched unmodified Aβ42 in height, tortuosity, length, secondary structure, and templating.
Liraglutide stood apart. Its KIP of 8.35 × 10⁻⁷ μM sits in the subpicomolar range, roughly 500,000-fold below semaglutide's, and at higher concentrations it also attenuated the growth phase. AFM showed that fibrils formed with a 10-fold excess of liraglutide were less mature, with a mean height of 2.9 nm against 4.4 nm for controls, and were longer and more tortuous, consistent with reduced secondary nucleation at fibril surface defects. The kinetic dual fit and an independent geometric argument from the fibril lengthening placed the secondary-nucleation potency, KIS, in agreement within an order of magnitude, near tens of micromolar and single-digit micromolar respectively. Liraglutide also lowered fibril templating, whether present during growth or added to preformed fibrils, and shrank the hydrodynamic radius of stabilized Aβ42 oligomers. Copelleting experiments kept all three active GLP-1RAs in the soluble fraction, arguing against simple monomer sequestration and for transient interactions with on-pathway intermediates. The parent peptide GLP-1(7-37) inhibited by a different route, suppressing elongation with a KIE near 0.77 μM.
The work places GLP-1RAs within the structure-activity-by-kinetics framework for Aβ42 inhibitors. Because secondary nucleation drives the autocatalytic production of cytotoxic oligomers, liraglutide's dual action makes it a candidate scaffold for optimization, by tuning the C16 fatty acid on Lys26 or by edits that cut size and hydrophobicity to aid blood-brain barrier entry. The clinical picture remains mixed, with the phase III evoke trials of oral semaglutide failing to slow AD while the smaller liraglutide trial showed benefit on secondary measures, and the authors stress that brain concentrations are still poorly defined. They note, however, that reported liraglutide brain levels approach the KIP measured here, leaving open whether direct inhibition of primary nucleation contributes to the protective signals seen in observational data and trials.